Eye Removal (Enucleation & Evisceration)
Removal of an eye may be required following a severe injury, to control pain in a blind eye, to treat some intraocular tumors, to alleviate a severe infection inside the eye, or for cosmetic improvement of a disfigured eye. Treatments Both surgeries are usually performed in the operating room under local anesthesia with sedation or general anesthesia.
Most patients go home the same day as surgery. Some patients will have a large pressure dressing or bandage placed on the eye for one week to prevent bleeding. You may be asked to take medications after surgery such as antibiotics, steroids, or pain-relievers. Patients may wear a patch after surgery for several days to several weeks, until they receive their prosthesis. Several weeks after surgery, an artificial eye, or prosthesis, is made by an ocularist. You can think of this as a very large, thick, and firm contact lens. The front surface of the artificial eye is custom painted to match the patient’s other eye. The back surface is custom molded to fit exactly in the eye socket for maximum comfort and movement. The prosthesis is easily removable, and may be removed as needed for cleaning. Most patients sleep with the prosthesis in place. A prosthesis lasts decades in many patients. The ocularist and surgeon should follow the patient up every 6-12 months to ensure that the socket is healthy. The socket may atrophy (shrink) with time. This loss of volume may lead to eyelid laxity or socket changes that may affect the fit of the prosthesis. Additionally, the prosthesis can irritate tissues on the back of the eyelid or the tissues on the surface of the implant. Your providers will monitor for these changes. Risks and Complications Your surgeon cannot control all the variables that may impact your final result. The goal is always to improve a patient’s condition but no guarantees or promises can be made for a successful outcome in any surgical procedure. There is always a chance you will not be satisfied with your results and/or that you will need additional treatment. As with any medical decision, there may be other inherent risks or alternatives that should be discussed with your surgeon. Eye Removal (Enucleation and Evisceration) Photos • Find an ASOPRS Surgeon Near You |
 Enucleation is the surgical removal of the entire eye. Evisceration is the surgical removal of the contents of the eye, leaving the white part of the eye (the sclera) and the eye muscles intact.
Enucleation is the surgical removal of the entire eye. Evisceration is the surgical removal of the contents of the eye, leaving the white part of the eye (the sclera) and the eye muscles intact.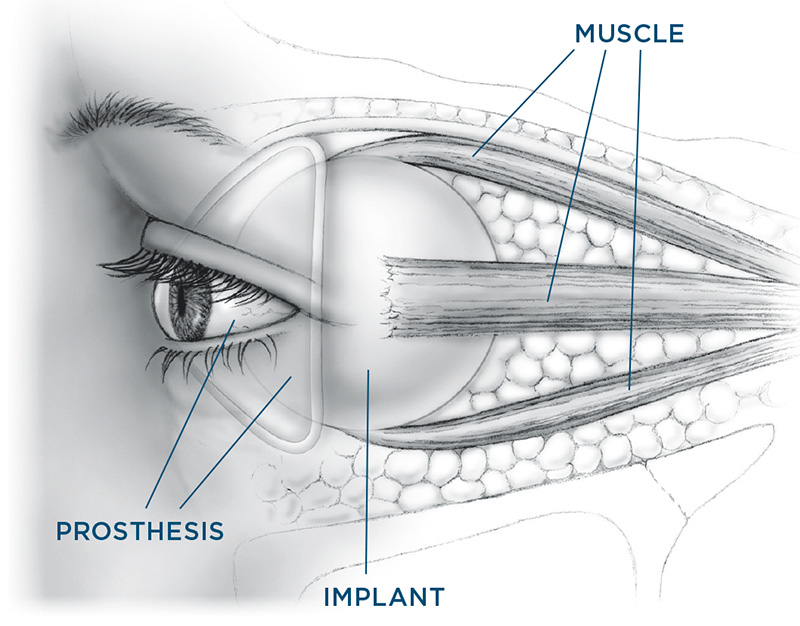 After enucleation or evisceration, most of the lost volume is replaced by a spherically shaped implant or fatty tissue from the patient’s own body placed in the eye socket. Implants can be made of a variety of materials including acrylic, hydroxyapatite, porous polyethyline, or dermis fat, among others. In most cases, the eye muscles are attached to the implant following enucleation, in order to preserve eye movement. Depending on availability, the implant may be wrapped with sclera from a cadaver (this tissue is thoroughly tested for diseases) to ease attaching muscles to the implant and to allow for a smooth surface interface with the patient’s own tissue that will cover the implant.
After enucleation or evisceration, most of the lost volume is replaced by a spherically shaped implant or fatty tissue from the patient’s own body placed in the eye socket. Implants can be made of a variety of materials including acrylic, hydroxyapatite, porous polyethyline, or dermis fat, among others. In most cases, the eye muscles are attached to the implant following enucleation, in order to preserve eye movement. Depending on availability, the implant may be wrapped with sclera from a cadaver (this tissue is thoroughly tested for diseases) to ease attaching muscles to the implant and to allow for a smooth surface interface with the patient’s own tissue that will cover the implant.